Authorization To Release Information Template
Authorization To Release Information Template - An authorization to release information form is a document that allows a healthcare provider to share a patient's protected health information (phi) with a designated third party, such as another medical provider, a personal representative, or a family member. Direct free access to pdf of hipaa release. A release of information form is a document that individuals can use when they would like to authorize another individual or an entity to use and release a certain type of their personal information. This document is essential in situations involving the privacy and confidentiality of personal or sensitive data. The authorization form for the release of patient information, akin to a parent information form, must include patient identification, the type of information to be released, purpose of disclosure, and the recipient’s details for lawful sharing. Here is a sample authorization letter to release information: I am aware that my withdrawal will not be effective as to uses and/or disclosures of my health information that the person and or agency listed above have already made in reference to this authorization. I grant permission for the release of the specified information as required. To obtain information on how to withdraw my authorization, i may contact the staff providing/coordinating my services. This form is for use when such authorization is required and complies with the health insurance portability and accountability act of 1996 (hipaa) privacy standards. Specific description of information authorized for release. The purpose of the document is to provide individuals or entities with legal consent from an individual for information disclosure. An authorization to release information form is a document that allows a healthcare provider to share a patient's protected health information (phi) with a designated third party, such as another medical provider, a personal representative, or a family member. Express authorization and consent for information release. The medical record information release (hipaa) form allows patients to give authorization to a 3rd party and access their health records. 72.5 kb ) for free. Understand that the information may/will include treatment for mental and/or physical illness, counseling or treatment for drug and/or alcohol abuse, human immunodeficiency virus (hiv), including acquired immunodeficiency syndrome (aids) or tests for hiv or aids. To obtain information on how to withdraw my authorization, i may contact the staff providing/coordinating my services. A patient can also request their medical records not currently in their possession. Always stay on top of your patient's health concerns, and safeguard their details with ease. Always stay on top of your patient's health concerns, and safeguard their details with ease. Express authorization and consent for information release. A medical records release authorization form is a document that allows a person to disclose protected health information to a third party. Dear [recipient’s name], i, [your name], hereby authorize [authorized person’s name] to request and receive any. When deciding to release an information from the government, start processing your authorization a month before you will need the authorized person to act for a transaction and use your data. An authorization to release information form is a document that allows a healthcare provider to share a patient's protected health information (phi) with a designated third party, such as. The purpose of the document is to provide individuals or entities with legal consent from an individual for information disclosure. 72.5 kb ) for free. I, [your name], hereby authorize [organization's name] to release my information, including but not limited to [specify information, e.g., medical, financial], to [recipient's name and address], for the purpose of [specify purpose, e.g., insurance claim,. A letter of authority to release information serves as a formal consent document that grants a designated person or entity the right to access specific information on your behalf. Once signed, you’ll automatically receive a finalized pdf — ready to download, print, and share. Clear statement of why the information is being released. This document is essential in situations involving. An authorization letter to release information is a legal document that gives permission to a third party to access and share an individual’s personal or protected information. Free immediate download of medical relasese form pdf. The authorization form for the release of patient information, akin to a parent information form, must include patient identification, the type of information to be. The purpose of the document is to provide individuals or entities with legal consent from an individual for information disclosure. A letter of authority to release information serves as a formal consent document that grants a designated person or entity the right to access specific information on your behalf. I grant permission for the release of the specified information as. Free immediate download of medical relasese form pdf. Clear statement of why the information is being released. The purpose of the document is to provide individuals or entities with legal consent from an individual for information disclosure. Dear [recipient’s name], i, [your name], hereby authorize [authorized person’s name] to request and receive any information related to [reason for request] on. A patient can also request their medical records not currently in their possession. What is an authorization to release information? It also allows the added option for healthcare providers to share information. Understand that the information may/will include treatment for mental and/or physical illness, counseling or treatment for drug and/or alcohol abuse, human immunodeficiency virus (hiv), including acquired immunodeficiency syndrome. I grant permission for the release of the specified information as required. Free immediate download of medical relasese form pdf. A patient can also request their medical records not currently in their possession. The authorization form for the release of patient information, akin to a parent information form, must include patient identification, the type of information to be released, purpose. A release of information form is a document that individuals can use when they would like to authorize another individual or an entity to use and release a certain type of their personal information. Always stay on top of your patient's health concerns, and safeguard their details with ease. I authorize ________________________ (“authorized party”) to use or disclose the following:. A letter of authority to release information serves as a formal consent document that grants a designated person or entity the right to access specific information on your behalf. 72.5 kb ) for free. Time period for which the authorization is valid. Express authorization and consent for information release. Powers granted under a medical release can be revoked or reassigned at any time. Here is a sample authorization letter to release information: Sample authorization for release of confidential information. A patient can also request their medical records not currently in their possession. This consent form will expire on (date)_____________ or __________ days from the date of service recipient signature, whichever date comes sooner. To obtain information on how to withdraw my authorization, i may contact the staff providing/coordinating my services. Once signed, you’ll automatically receive a finalized pdf — ready to download, print, and share. Clear statement of why the information is being released. The authorization form for the release of patient information, akin to a parent information form, must include patient identification, the type of information to be released, purpose of disclosure, and the recipient’s details for lawful sharing. Download or preview 1 pages of pdf version of authorization to release information (doc: An authorization to release information form is a document that allows a healthcare provider to share a patient's protected health information (phi) with a designated third party, such as another medical provider, a personal representative, or a family member. Hire a legal lawyer to guide you through the process.
10+ Authorization to Release Information Template room

Authorization to Release Information Fill Out, Sign Online and
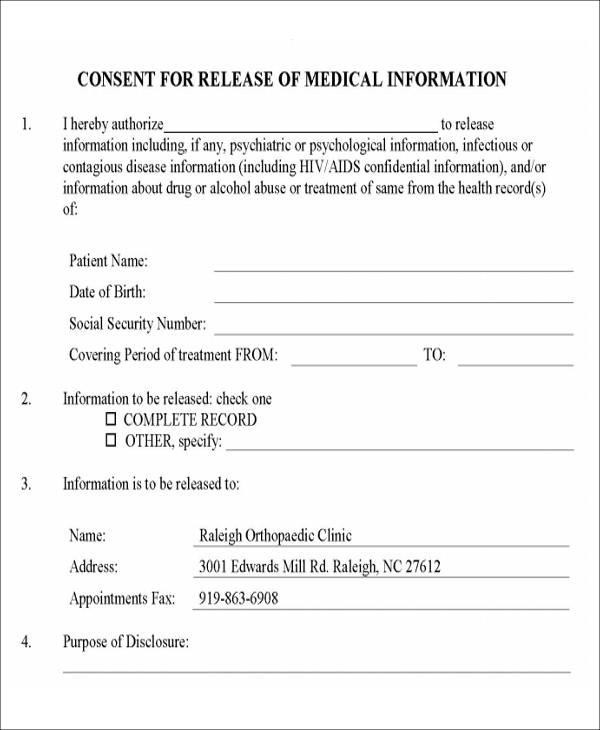
FREE 9+ Release Of Medical Information Form Samples in MS Word PDF
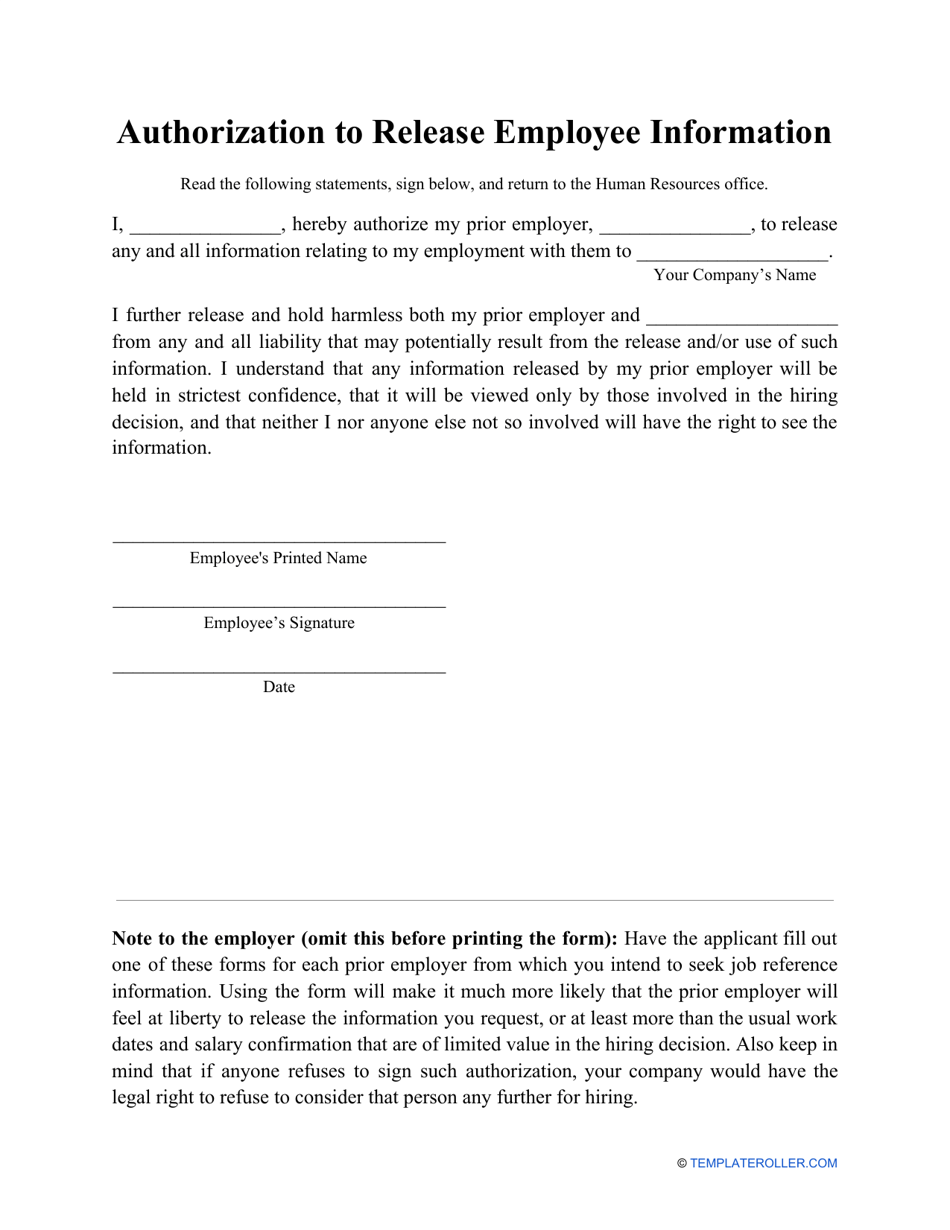
Authorization to Release Employee Information Form Fill Out, Sign

Consent To Release Information Form Template Printable Word Searches
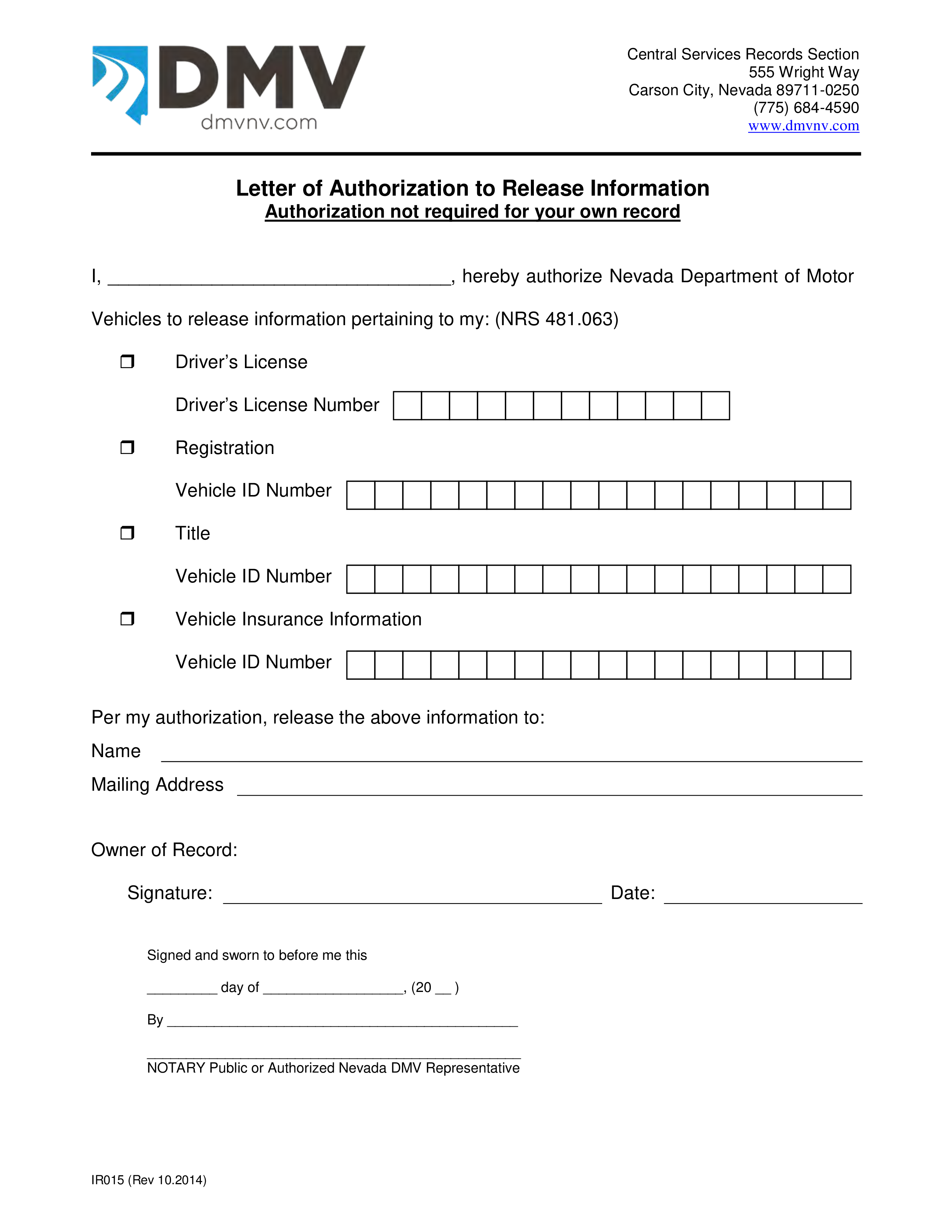
Letter Of Authorization To Release Information Templates at
FREE 40+ Release Forms in PDF Excel MS Word
Authorization to Release Account Information Template in Word, Pages

Release Of Information Forms Printable (BLANK TEMPLATE)
Distribution Authorization Letter
The Purpose Of The Document Is To Provide Individuals Or Entities With Legal Consent From An Individual For Information Disclosure.
Understand That The Information May/Will Include Treatment For Mental And/Or Physical Illness, Counseling Or Treatment For Drug And/Or Alcohol Abuse, Human Immunodeficiency Virus (Hiv), Including Acquired Immunodeficiency Syndrome (Aids) Or Tests For Hiv Or Aids.
This Form Is For Use When Such Authorization Is Required And Complies With The Health Insurance Portability And Accountability Act Of 1996 (Hipaa) Privacy Standards.
A Medical Records Release Authorization Form Is A Document That Allows A Person To Disclose Protected Health Information To A Third Party.
Related Post: